Minimizing Human Error in Dental Sedation: Crisis Management and Airway Preparedness
 Sedation and Anesthesia Education
Sedation and Anesthesia Education 
Medical emergencies in the dental office are inherently low-frequency events. Because a well-managed sedation practice rarely encounters a critical crisis, maintaining clinical competence in emergency response requires deliberate, proactive preparation. When an adverse event does occur, the transition from routine care to crisis management happens in seconds. Clinicians must be equipped not only with technical knowledge but also with structural strategies to manage cognitive overload and ensure patient safety.
The Reality of Hindsight Bias in Clinical Crises
Reviewing emergency case studies in a calm, non-stressed environment often leads to a phenomenon known as hindsight bias. From an external perspective, the correct diagnostic and therapeutic choices seem obvious, creating a misperception that real-time crises offer simple, linear paths to success.
In reality, active emergencies generate intense psychological pressure. Simple technical mishaps—such as a dislodged monitor lead during a sudden bradycardic episode—can easily be misinterpreted as a catastrophic shift into asystole because the clinical environment becomes chaotic very quickly. Recognizing that human error is the primary variable in perioperative complications highlights the necessity of systematic crisis management protocols.
Implementing Crew Resource Management (CRM)
To mitigate cognitive errors during high-stress events, the dental profession looks to high-reliability industries like aviation, adapting Cockpit Resource Management into Crew Resource Management (CRM). CRM focuses on the non-technical skills required to manage a clinical crisis effectively.
Key components of an effective CRM framework in the dental operatory include:
- Designating a Clear Team Leader: One clinician must maintain situational awareness, direct the team, and avoid getting bogged down in manual tasks.
- Clear Role Allocation and Workload Distribution: Every auxiliary staff member must know exactly what equipment to retrieve, which vitals to monitor, and when to call emergency services.
- Approachability and Flat Hierarchies: An emergency environment must allow auxiliary staff to voice concerns without fear of reprisal. If an assistant notices a subtle change in patient status, the operational culture must encourage them to speak up instantly.
The Crucial Role of Cognitive Aids
Because the human brain experiences narrow focus and memory degradation under acute stress, cognitive aids have become the core component of managing perioperative crisis events. Relying purely on memory to calculate emergency drug dosages or sequential algorithms is a risk to patient safety.
Clinicians should maintain both digital and physical cognitive aids within their emergency setups:
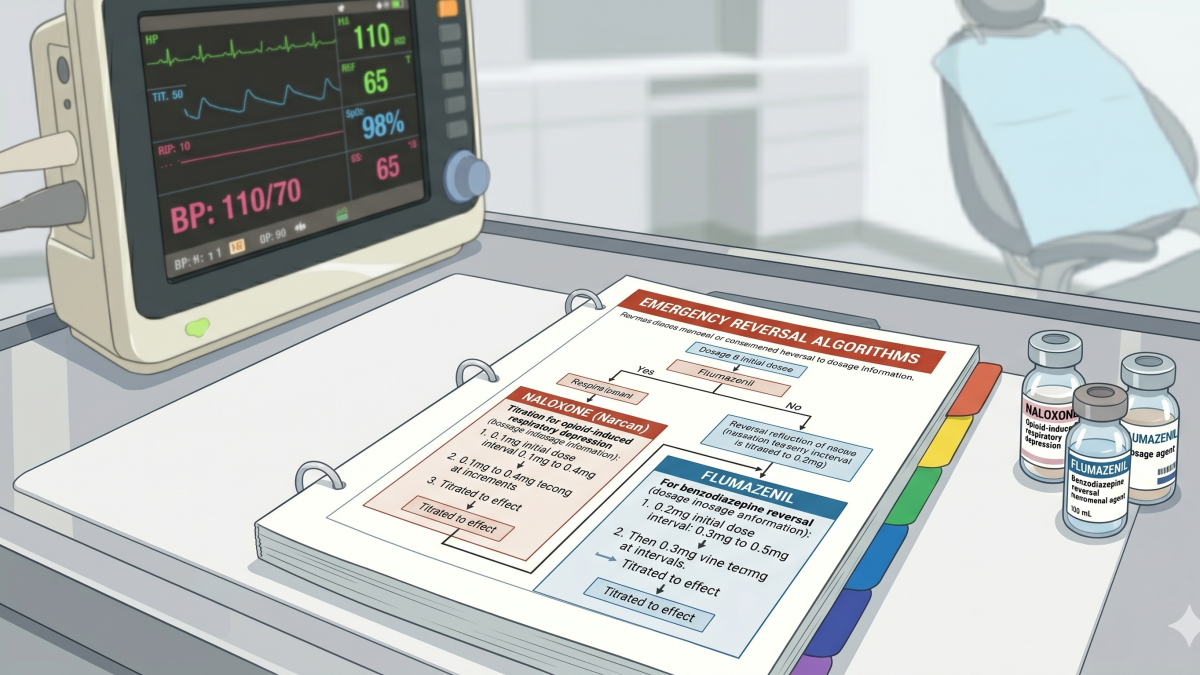
- Emergency Manuals: Keeping printed, tabbed emergency workflows (such as the Stanford Emergency Manual) directly on the sedation crash cart ensures that immediate action plans are visible to the entire team.
- Interactive Applications: Utilizing specialized emergency applications allows dental teams to input a patient’s metrics ahead of time to receive instant, accurate drug dosages and step-by-step algorithms during an emergency.
Managing Sedation Airway Emergencies
The vast majority of critical sedation emergencies center around the airway. Whether managing moderate or pediatric sedation, maintaining a patent airway is the single most vital component of patient stability.
1. Upper Airway Obstruction The most common complication of deeper levels of sedation is upper airway obstruction, typically caused by the tongue falling back against the posterior pharynx. This is especially prevalent in pediatric patients with hypertrophic tonsils or adenoids.
- Identification: Paradoxical chest movement ("bucking" or rocking chest patterns), sternal retractions, and a loss of capnography waveforms.
- Intervention: Immediate execution of the triple airway maneuver (head tilt, chin lift, and jaw thrust). If positional changes fail, an appropriately measured oropharyngeal airway (OPA) or nasopharyngeal airway (NPA) must be placed immediately to mechanically bypass the tongue.
2. Laryngospasm Laryngospasm is an involuntary, protective closure of the glottic opening mediated by the internal branch of the superior laryngeal nerve. It is often triggered by secretions, blood, or debris irritating the vocal cords during a light plane of sedation.
- Identification: High-pitched inspiratory stridor or complete silence accompanied by intense accessory muscle use and rapidly dropping oxygen saturation (SpO2).
- Intervention: Remove the surgical stimulus, clear the airway of debris via suction, and apply continuous positive pressure with 100% oxygen using a bag-valve-mask (BVM). Concurrently, firm digital pressure should be applied to the laryngospasm notch (located behind the lobule of the ear, anterior to the mastoid process) to elicit a painful stimulus and break the reflex.
3. Bronchospasm An acute asthmatic attack or bronchospasm involves the constriction of smooth muscle around the lower airways, preventing gas exchange.
- Identification: Expiratory wheezing, increased ventilatory resistance, and a downward trend in SpO2.
- Intervention: Administer a fast-acting bronchodilator (such as albuterol) via a spacer or deliver positive-pressure oxygen. If the bronchospasm is severe and unresponsive to inhaled agents, intramuscular or subcutaneous epinephrine remains the gold standard to achieve rapid bronchodilation.
Emergency Reversals in Over-Sedation
When a patient transitions into an unintended deeper plane of sedation where they no longer respond purposefully to verbal commands, the dental team must immediately stop the procedure and prepare to reverse the causative agents if the airway becomes unstable.
- Benzodiazepine Reversal (Flumazenil): Administered in incremental doses of 0.2 mg to 0.5 mg titration steps to safely reverse respiratory depression without triggering acute withdrawal or seizures.
- Opioid Reversal (Naloxone): Administered to counteract opioid-induced respiratory depression, titrated carefully to restore spontaneous ventilation while balancing patient comfort.
Ultimately, predictable outcomes in dental anesthesia depend on early recognition, structured teamwork, and the immediate utilization of cognitive aids. By establishing robust emergency protocols and practicing team-based simulations, dental practitioners ensure that rare crisis events are met with decisive, systematic, and life-saving care.
Learn more about advanced airway management and safety protocols at https://www.isedatesafe.com
Categories: : Patient Safety, Sedation Anesthesia