Navigating the Esoteric Nuances of Local Anesthesia Pharmacology
 Sedation and Anesthesia Education
Sedation and Anesthesia Education 
Local anesthesia is the absolute benchmark of compassionate care in dental practice. While every clinician administers these agents routinely, the underlying pharmacology features intricate nuances that directly dictate clinical success and patient safety.
Moving past the absolute basics opens up a deeper understanding of how subtle chemical variances can shift a predictable procedure into a clinical challenge. By evaluating the specific pharmacokinetics of these agents, practitioners can refine their clinical decisions and optimize local anesthesia outcomes.
The Chemistry of Local Anesthesia Action
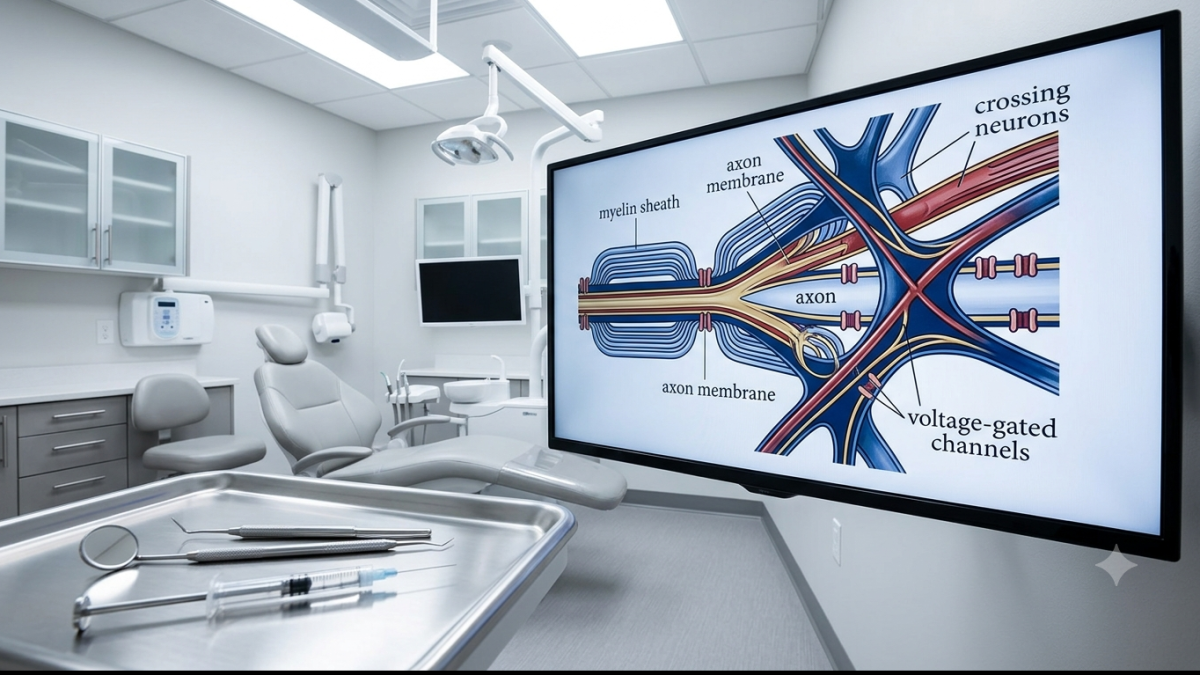
At its core, a local anesthetic functions as a sodium channel blocker. The molecule must pass through the nerve membrane to clog the sodium channel from the intracellular side, effectively stopping the influx of sodium ions and halting the propagation of the action potential.
However, the journey of the drug from the syringe to the inside of the nerve axon relies heavily on two critical chemical parameters: the dissociation constant (pKa) and lipid solubility.
The Role of pKa and Tissue pH
The pKa of a drug represents the pH at which 50% of the drug exists in an ionized state and 50% in an un-ionized state. This distinction is vital because only the un-ionized form of the drug can cross the lipid-rich nerve membrane. Once inside the cell, a portion of the drug re-ionizes to bind to the sodium channel receptor.
Healthy body tissues typically maintain a pH of 7.4. When an anesthetic like articaine (pKa = 7.8) is deposited, approximately 29% of the drug remains un-ionized and available to cross the membrane, leading to a rapid onset of 2 to 4 minutes.
Conversely, bupivacaine features a higher pKa of 8.1. At a normal tissue pH, only about 18% of the drug is un-ionized, resulting in a noticeably slower onset of action.
The Problem with Infected Tissues
Local anesthetics lose significant efficacy in the presence of infection due to the localized drop in tissue pH toward an acidic environment (often around 6.0). In an acidic environment, weak bases become heavily ionized.
For instance, at a pH of 6.0, the un-ionized fraction of an anesthetic can plummet from 29% down to just 1.6%. Because nearly the entire dose becomes trapped in the ionized state extracellularly, it cannot penetrate the nerve sheath, explaining the classic difficulty in achieving profound anesthesia in infected areas.
Balancing Potency and Duration of Action
Predictable sedation and pain management require matching the specific properties of an anesthetic to the procedural needs.
- Potency is primarily governed by the drug's lipid solubility. Highly lipid-soluble agents penetrate membranes more efficiently, requiring a lower concentration gradient to drive the molecule to its site of action. This explains why bupivacaine is highly effective at a 0.5% concentration, whereas articaine is administered at 4%.
- Duration of action is tied directly to protein binding capacity. Anesthetics that bind tightly to the proteins within the receptor site resist vascular washing and subsequent metabolism.
Local Anesthetic Comparison Profile
- Articaine
- Lidocaine
- Bupivacaine
Articaine holds a unique position due to its molecular structure, containing both an ester and an amide moiety. This allows it to undergo rapid biotransformation primarily via plasma cholinesterases, resulting in an exceptionally short half-life of 20 minutes and minimizing systemic drug accumulation.
Recognizing and Preventing Systemic Toxicity
Systemic toxicity represents the most significant acute risk associated with local anesthetics. High plasma concentrations can trigger severe central nervous system (CNS) and cardiovascular complications, often exacerbated by inadvertent intravascular injection.
The Progression of Local Anesthetic Overdose
Systemic toxicity typically manifests on a continuum related to serum levels:
- Low Levels: Minor antiarrhythmic benefits (specifically with lidocaine).
- Early Toxicity: Lightheadedness, tinnitus, blurred vision, circumoral or tongue numbness, and muscle twitching.
- Advanced Toxicity: Tonic-clonic convulsions, unconsciousness, respiratory depression, and eventual cardiovascular collapse.
Highly protein-bound agents like bupivacaine pose an elevated cardiovascular risk. An overdose can induce profound myocardial depression and total heart block, which are notoriously difficult to resuscitate.
Advanced Reversal with Intralipid Therapy
While traditional emergency management focuses on immediate airway protection, oxygenation, and seizure control via benzodiazepines, true systemic toxicity requires clearing the plasma concentration.
Modern emergency preparedness incorporates intralipid therapy (a 20% intravenous fat emulsion) as a rescue agent for local anesthetic overdose.
Clinical Note: Intralipid acts as a "lipid sink," creating micelles that encapsulate the lipophilic anesthetic molecules in the bloodstream. This prevents them from crossing the blood-brain barrier or binding to cardiac receptors, accelerating clearance from vital organs.
Clinical Screening and Drug Interactions
Achieving predictable outcomes requires adapting maximum recommended dosages to individual patient profiles. Age, hepatic health, and concurrent medications alter how these drugs behave systemically.
- Beta-Blockers and Amiodarone: These medications compete for the same hepatic metabolic pathways as amide anesthetics. For patients taking non-selective beta-blockers, the total anesthetic dose should be reduced conservatively to prevent elevated plasma levels and unexpected hypertensive reactions due to unopposed alpha-receptor stimulation.
- Pediatric Precautions: Articaine is cleared for pediatric patients aged 4 and older, with a reduced maximum dose recommendation of 5 mg/kg (compared to the adult 7 mg/kg specification).
- Methemoglobinemia Risks: Particular attention must be paid to agents capable of inducing methemoglobinemia, a condition where hemoglobin is oxidized into a state that cannot release oxygen to peripheral tissues. Prilocaine and benzocaine are the primary culprits. Practitioners should look for a hallmark drop in pulse oximetry that stabilizes artificially at 85%, accompanied by cyanosis or chocolate-colored blood.
Maintaining a deep understanding of these advanced pharmacological principles ensures that pain control remains both highly effective and structurally safe for every patient in the chair.
To review comprehensive clinical safety guidelines or explore advanced training in sedation pharmacology, visit https://www.isedatesafe.com.
Categories: : Sedation Anesthesia