Navigating the Sedation Continuum: Avoiding the "Cookbook" Trap in Dental Anesthesia
 Sedation and Anesthesia Education
Sedation and Anesthesia Education 
The dental operatory can be an unpredictable environment, especially when introducing sedative agents. A common pitfall in clinical practice is the temptation to standardize—or "cookbook"—the approach to sedation. It is easy to treat a sedation case the same way as the last hundred cases, but in anesthesia, relying on uniform protocols rather than individual patient responses is a significant clinical risk.
Because every patient possesses a unique physiological makeup, treating everyone identically can lead to unintended deep sedation or rescue situations. Safe practice requires a thorough understanding of the sedation continuum, accurate patient assessment, and a commitment to clinical customization.
The Sinusoidal Nature of the Sedation Continuum
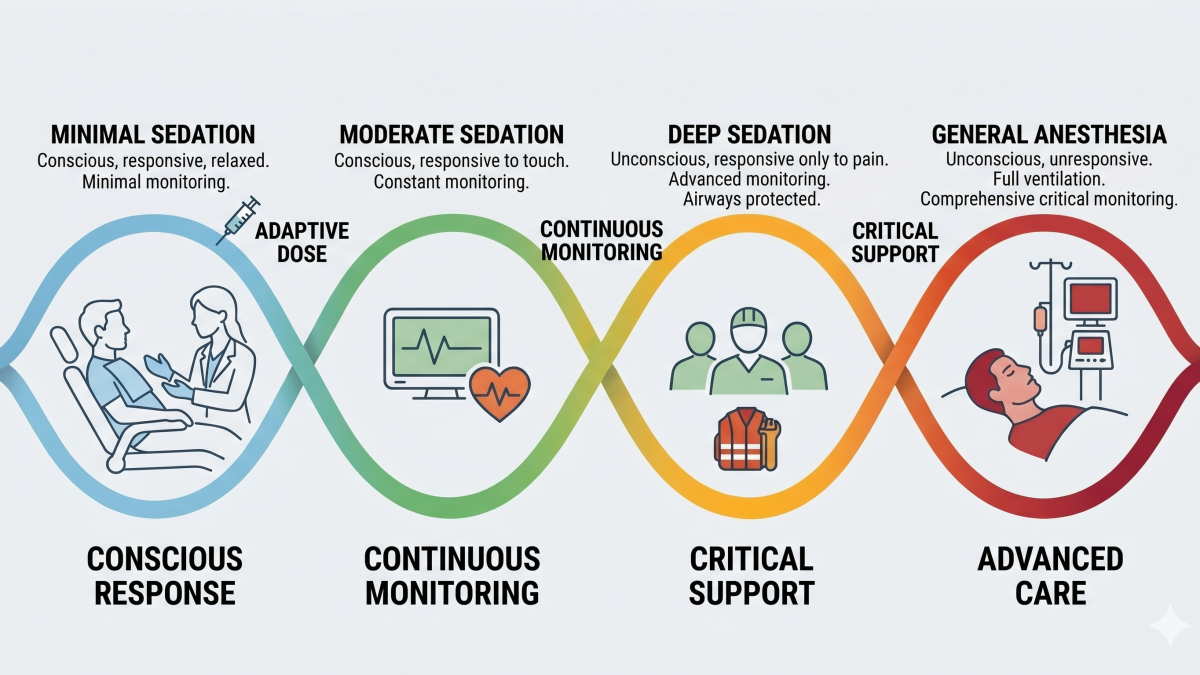
The sedation continuum does not operate in distinct, isolated compartments; instead, it behaves like a dynamic wave, constantly shifting based on drug absorption, redistribution, and individual patient sensitivity. The American Society of Anesthesiologists (ASA) and the American Dental Association (ADA) define four distinct levels within this continuum:
- Minimal Sedation: A drug-induced state during which patients respond normally to verbal commands. Cognitive function and coordination may be impaired, but ventilatory and cardiovascular functions remain unaffected.
- Moderate Sedation: A deeper state where patients respond purposefully to verbal commands, either alone or accompanied by light tactile stimulation. No airway interventions are typically required.
- Deep Sedation: A state where patients cannot be easily aroused but respond purposefully following repeated or painful stimulation. The ability to independently maintain ventilatory function may be impaired.
- General Anesthesia: A drug-induced loss of consciousness during which patients are not arousable, even by painful stimulation. Airway maintenance and positive-pressure ventilation are frequently required.
Every patient responds differently to sedative drugs. For example, a standard titration of nitrous oxide might provide mild relaxation for one individual, while placing another patient into a deep plane of sedation. Clinicians must monitor the patient’s actual responsiveness rather than relying solely on the administered dose, ensuring they possess the skills necessary to rescue a patient from a deeper plane of sedation than intended.
Moving Beyond the "Cookbook" Approach
The temptation to standardize clinical techniques is common in routine restorative dentistry, but applying a rigid framework to sedation pharmacology can compromise patient safety.

A patient's physiological response is influenced by a multitude of variables, including age, weight, metabolic rate, emotional maturity, and underlying systemic health. A standard dose that provides predictable results in a healthy adult may cause prolonged respiratory depression or paradoxical excitation in a pediatric or geriatric patient.
Clinicians must tailor the pharmacological approach to each individual case. This involves evaluating the patient's anxiety levels, clinical needs, and medical history to select the most appropriate agent or combination of agents, rather than relying on a single, fixed protocol for every appointment.
Patient Selection and Systemic Risk Factors
Accurate patient evaluation prior to the day of surgery is essential for mitigating risks. Relying on the ASA Physical Status Classification system helps clinicians communicate health status and determine whether a patient is a suitable candidate for in-office sedation:
- ASA I: Normal, healthy patient; non-smoker with minimal alcohol use. Ideal candidate for standard minimal or moderate sedation protocols.
- ASA II: Patient with mild systemic disease (e.g., well-controlled hypertension or type 2 diabetes). Suitable for office-based sedation; requires minor protocol adjustments.
- ASA III: Patient with severe systemic disease that limits activity (e.g., poorly controlled diabetes or metabolic syndrome). High risk; requires careful titration, extended monitoring, or medical consultation.
- ASA IV: Patient with severe systemic disease that is a constant threat to life. Generally contraindicated for elective in-office dental sedation.
Evaluating high-risk systemic conditions, such as metabolic syndrome or undiagnosed obstructive sleep apnea (OSA), is crucial during the pre-operative workup. Conditions like a high BMI or an advanced neck circumference significantly increase the likelihood of airway obstruction under sedation. Tools like the STOP-BANG questionnaire help identify undiagnosed airway risks before administering sedatives.
Clinical Application and Adverse Outcomes
In dental anesthesia, adverse outcomes are rarely caused by a single factor; instead, they typically result from unrecognized airway compromise that progresses to cardiovascular collapse. When a patient transitions deeper into the sedation continuum, the tongue can fall backward, creating an acute upper airway obstruction.
Airway Obstruction ──> Hypoxia ──> Hypercapnia ──> Cardiovascular Collapse
Maintaining safety relies on constant vigilance and monitoring. Clinicians cannot afford to look away or focus exclusively on the dental procedure. Team members must be trained to recognize the early signs of airway compromise—such as grunting, snoring, or a drop in oxygen saturation—and respond immediately with corrective maneuvers like a jaw thrust or head tilt.
Furthermore, pre-operative instructions, including NPO (fasting) guidelines, must be strictly enforced. If a patient inadvertently drifts from moderate to deep sedation, intact airway protective reflexes can be compromised. Adhering to proper fasting protocols helps prevent vomiting and silent aspiration, protecting the patient's airway throughout the peri-operative period.
Conclusion
Safe dental sedation requires a move away from rigid, formulaic dosing. Every clinical case demands a dedicated evaluation, custom drug titration, and active monitoring of real-time patient responses. By understanding the fluid nature of the sedation continuum and treating every patient as an individual case, dental teams can achieve predictable clinical outcomes while maintaining high standards of patient safety.
To deepen your clinical knowledge and ensure compliance with regional sedation requirements, explore the advanced continuing education programs and safety resources available at Sedation and Anesthesia Education.
Categories: : Patient Safety, Sedation Anesthesia