Using ASA Classification and Medical History to Improve Sedation Safety in the Dental Office
 Sedation and Anesthesia Education
Sedation and Anesthesia Education 
Before any sedative drug is administered, the most important clinical decision has already been made: whether the patient is an appropriate candidate for sedation in the first place.
That decision depends largely on how well the provider evaluates medical history, assigns ASA classification correctly, and recognizes when treatment belongs in a different setting. These steps are not just paperwork—they are some of the strongest predictors of sedation safety.
A structured pre-sedation evaluation helps reduce complications, supports better outcomes, and ensures that dental providers are working within an appropriate risk profile for office-based care.
Sedation Safety Begins with Patient Selection
Every sedation appointment starts with a question: Is this patient appropriate for office-based sedation today?
Answering that requires more than reviewing a chart from a prior visit. It means gathering complete medical history information, updating findings on the day of treatment, and performing a focused physical evaluation before proceeding.
Risk exists whenever sedation is delivered. The purpose of pre-sedation assessment is not to eliminate risk entirely—it is to reduce the likelihood of adverse events by identifying patients who may require additional preparation, consultation, stabilization, or referral.
Providers who consistently follow structured assessment protocols make safer sedation decisions and are better positioned to respond appropriately when conditions change.
Why ASA Classification Still Matters in Dentistry
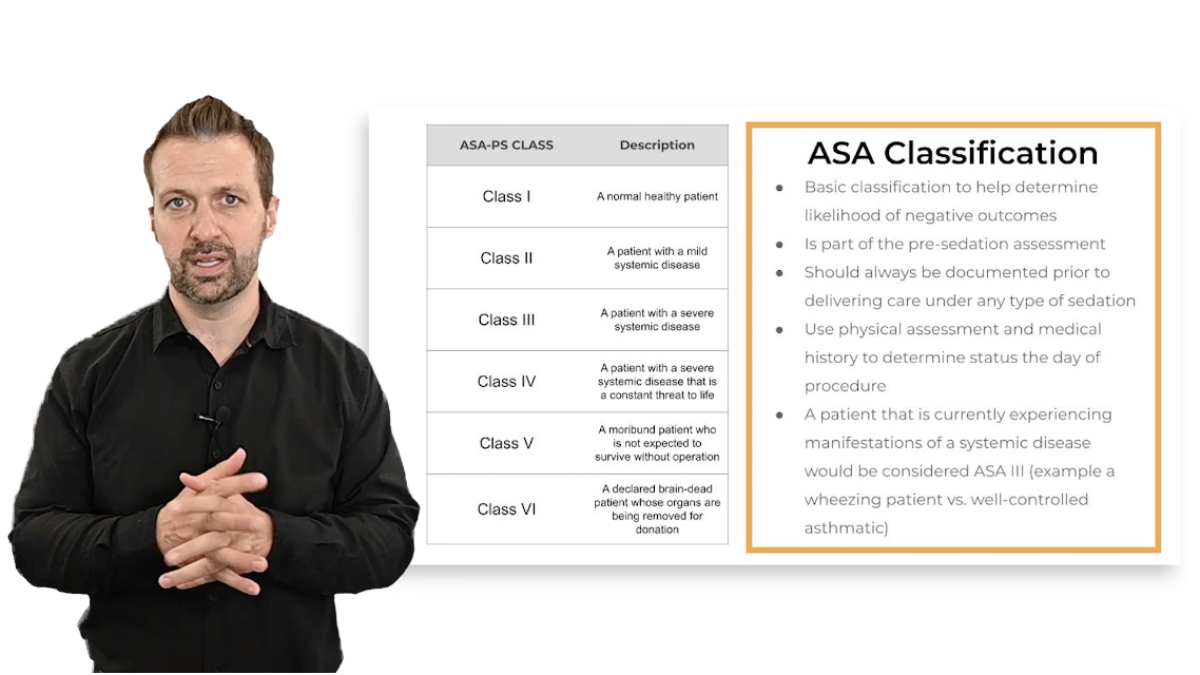
The American Society of Anesthesiologists (ASA) classification system has been used since the 1940s to estimate medical risk associated with anesthesia and sedation. It remains one of the most practical tools dental providers have for determining whether treatment should occur in an office or hospital environment.
In most dental sedation settings, appropriate candidates typically fall into:
- ASA I (healthy patients)
- ASA II (mild systemic disease that is well controlled)
Patients classified as ASA III or higher often require additional medical management before sedation—or treatment in a hospital-based environment.
This distinction matters because outcome data consistently show that higher ASA classifications are associated with increased complication rates during sedation and anesthesia procedures.
Recognizing when a patient falls outside the safe range for office-based sedation is one of the most important protective decisions a provider can make.
Medical Conditions Are Not Static on the Day of Treatment
One of the most overlooked steps in sedation evaluation is reassessing the patient’s medical condition on the day of the procedure.
ASA classification is not permanent. It reflects current medical stability, not historical diagnosis alone.
For example:
A patient with well-controlled asthma may be classified as ASA II during the consultation visit. But if that same patient presents on the day of sedation with active wheezing or respiratory symptoms, their classification changes—and so should the treatment plan.
Similarly, patients with poorly controlled diabetes, uncontrolled hypertension, or active respiratory illness may temporarily shift into a higher-risk category.
Day-of-procedure reassessment helps prevent sedation from proceeding under conditions that increase complication risk.
Case-Based Risk Assessment Improves Clinical Judgment
Understanding ASA classification becomes easier when applied to real clinical scenarios.
Consider a patient with Type 2 diabetes who presents for moderate sedation. If laboratory values and medical history suggest poor glycemic control, that patient may no longer qualify as ASA II—even if they are taking medication.
In those cases, postponing treatment until the condition is better managed reduces the risk of intraoperative complications.
By contrast, a patient taking medication for ADHD with otherwise normal vital signs and physical findings would typically remain within ASA II classification and may be appropriate for office-based sedation.
These types of distinctions are routine in sedation practice and highlight why classification depends on current stability, not diagnosis alone.
When Medical Consultation Becomes Necessary
Certain conditions almost always justify consultation before proceeding with sedation.
These commonly include:
- Cardiac conditions or prior cardiac repairs
- Respiratory disease requiring emergency care history
- Liver dysfunction
- Kidney disease
- Cancer treatment history
- Psychiatric medication use affecting sedation response
- Recent major surgery
- Orthopedic hardware placement
- Complex medication regimens
Parents and patients are not always reliable historians when it comes to medical details. Direct consultation with physicians or specialists helps confirm stability and reduces uncertainty before sedation begins.
This step is especially important when medications with sedative or psychoactive effects may interact with planned anesthetic agents.
Why Social History Should Never Be Skipped
Alcohol use and substance exposure directly affect sedation pharmacology.
Heavy alcohol use can interfere with hepatic metabolism of sedative medications. Because many commonly used agents depend on liver processing, impaired metabolism may lead to prolonged sedation or unexpected drug effects.
For that reason, social history should be treated as part of routine sedation evaluation—not an optional addition.
Even mild details about smoking status, alcohol intake, or medication adherence can change risk classification and treatment planning.
Fasting Guidelines Are a Core Part of Risk Reduction
Pre-sedation fasting instructions are based on decades of evidence showing reduced aspiration risk when gastric contents are minimized before anesthesia.
Typical fasting recommendations include:
- Clear liquids: stop 2 hours before sedation
- Breast milk: stop 4 hours before sedation
- Infant formula or milk: stop 6 hours before sedation
- Fatty meals or meat: stop at least 8 hours before sedation
These timelines apply broadly across age groups and are designed to reduce the likelihood of aspiration complications during procedural sedation.
However, they do not guarantee complete gastric emptying. Instead, they represent evidence-based intervals associated with lower complication rates.
Patients with diabetes or metabolic conditions may require individualized fasting instructions coordinated with their physician.
Younger Patients Require Additional Caution
Age also influences sedation risk.
Very young pediatric patients—particularly those under age three—experience higher rates of respiratory complications during sedation. Combined with higher ASA classifications, this group represents one of the most vulnerable sedation populations.
Careful patient selection, enhanced monitoring, and appropriate setting decisions are especially important when treating younger children.
Office-Based Sedation Requires Strong Team Preparation
Sedation in dentistry differs from many medical environments because providers often perform both the procedure and sedation monitoring simultaneously.
That reality increases the importance of:
- strong patient selection protocols
- clear documentation
- appropriate consultations
- trained support staff
- reliable monitoring systems
Maintaining these safeguards supports safe sedation delivery and helps address concerns sometimes raised by medical colleagues regarding office-based anesthesia environments.
Thousands of dental sedation procedures are performed safely each day across the country. Consistent adherence to evaluation protocols plays a major role in making that possible.
Careful Assessment Prevents Most Sedation Complications
Sedation safety begins long before medications are administered.
Accurate ASA classification, updated medical history review, appropriate consultation, and proper fasting preparation all contribute to safer treatment decisions. When providers approach patient selection thoughtfully, they reduce the likelihood of complications and improve outcomes across every sedation level.
More clinical guidance and continuing education resources for sedation providers are available at: